Drug development is often portrayed as a story of discovery and innovation, but behind every promising molecule lies a critical question: what is the first safe dose in humans? Getting this wrong can derail years of research, cost millions, and, more importantly, put human lives at risk. Toxicology data forms the backbone of this decision, guiding scientists from animal studies to first-in-human (FIH) clinical trials with precision and caution.
Why First-in-Human Dose Selection Matters
Developing a new drug, whether a small molecule or a biologic, is a high-risk endeavor. One of the most frequent reasons for failure in Phase 1 clinical trials is inappropriate dose selection, accounting for nearly 30–40% of early clinical failures. An underestimated dose may show no efficacy, while an overestimated one can trigger severe toxicity.
To avoid these outcomes, toxicologists rely on scientifically grounded approaches to determine the Maximum Recommended Starting Dose (MRSD) for FIH studies. This ensures that new therapies enter human testing safely, ethically, and effectively, balancing patient protection with therapeutic potential.
Approaches Used to Determine the FIH Dose
Several scientific strategies are available to estimate a safe starting dose in humans. Commonly used methods include:
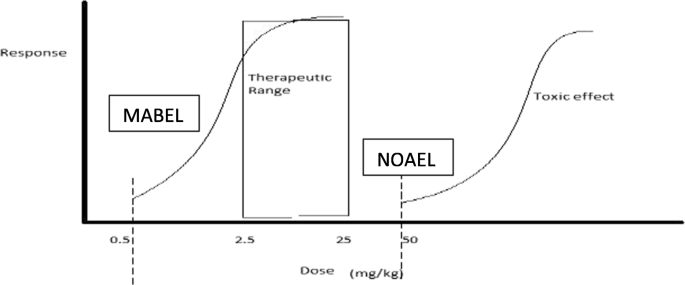
- Dose-by-factor approach based on No Observed Adverse Effect Level (NOAEL)
- Pharmacokinetically guided dose estimation
- Minimum Anticipated Biological Effect Level (MABEL)
- Pharmacokinetic-pharmacodynamic (PK-PD) modeling
- Use of data from similar drugs
- Microdosing studies
When these approaches yield different estimates, regulatory best practice dictates that the lowest calculated dose should be selected as the MRSD. For new chemical entities (NCEs) with limited data, the dose-by-factor approach is most commonly applied, though it is adapted depending on the nature of the therapeutic agent.
Foundational Toxicology Data Before FIH Studies
Before translating animal data to humans, robust toxicology studies are essential. Regulatory guidance recommends:
- Repeat-dose toxicology studies (typically 28 days)
- Conducted in one rodent species (such as rat or mouse)
- And one non-rodent species (dog, monkey, or minipig), chosen for metabolic relevance to humans
For large molecules and biologics, studies are performed in pharmacologically relevant species, those that express the human target and demonstrate comparable biological responses. In some cases, a single relevant species may suffice.
These studies typically identify the NOAEL, defined as the highest dose that does not cause a meaningful increase in adverse effects compared with controls. For biologics, toxicities are often linked to exaggerated pharmacology or the intended mechanism of action rather than off-target effects.
Translating Animal NOAEL to Human Equivalent Dose (HED)
Because animals and humans process drugs differently, direct dose conversion is unreliable. Instead, toxicologists calculate the Human Equivalent Dose (HED) using scientifically validated scaling methods.
Small Molecules
For small-molecule drugs, HED is calculated using body surface area (BSA) scaling, as recommended by regulatory authorities. Each species has a defined conversion factor that accounts for physiological differences, allowing animal doses (mg/kg) to be translated into human-relevant values.
Biologics
For biologics such as monoclonal antibodies:
- The HED is often assumed to be the same on a mg/kg basis
- Additional considerations include:
- Target-mediated drug disposition
- Complexity of the biological target (soluble vs. membrane-bound)
- Receptor occupancy and in vitro pharmacodynamic data
Emerging biologic platforms, such as cell-penetrating conjugates,may require alternative and evolving approaches to HED determination.
Oligonucleotides
Dose translation depends on the route of administration:
- IV or SC dosing: HED is based on BSA
- Intrathecal dosing: Calculated using cerebrospinal fluid (CSF) volume assumptions (approximately 15 mL in monkeys and 150 mL in humans)
From HED to Maximum Recommended Starting Dose (MRSD)
Once the HED is determined, a default 10-fold safety factor is applied to account for uncertainty. This margin may be increased if:
- Toxicities are severe or irreversible
- There is a steep dose-response curve
- Human target potency exceeds that seen in animal species
- Bioavailability differs significantly between species
Typically, the MRSD is set at one-tenth or less of the HED derived from the most sensitive species.
Real-World Examples of MRSD Calculation
1. Small Molecules (Non-Oncology)
The calculation follows this logic:
NOAEL ÷ species conversion factor = HED
HED ÷ safety factor × human body weight = MRSD
For example, if a dog NOAEL is 20 mg/kg, the resulting MRSD is 60 mg per day for humans after applying appropriate conversion and safety factors.
2. Oncology Drugs
Cancer therapeutics follow a modified approach to avoid under-dosing patients with advanced disease.
- Toxicologists determine:
- Highest Non-Severely Toxic Dose (HNSTD) in large animals
For oncology drugs:
- A 6-fold safety factor (instead of 10) is often applied
- This allows for a higher, yet controlled, Safe Starting Dose (SSD)
For example, with a dog NOAEL of 5 mg/kg and an HNSTD of 20 mg/kg, the resulting SSD may reach 120 mg. This approach reflects the ethical need to provide potentially effective doses to cancer patients.
3. Biologics (Monoclonal Antibodies)
For biologics:
- The most sensitive species (often monkeys) is selected
- NOAEL is not converted to HED
- Instead, a 10-fold safety factor is applied directly
Example:
- Monkey NOAEL: 30 mg/kg
- MRSD: 3 mg/kg
Key Takeaways
Determining the first-in-human dose is one of the most complex and responsibility-laden steps in drug development. While uncertainty is unavoidable, it can be mitigated through:
- Careful selection of dose-estimation methods
- Integration of model-based and empirical approaches
- Deep understanding of compound-specific biology and toxicology
A well-justified FIH dose not only protects trial participants but also lays the foundation for clinical success.
Insights
In early drug development, safety is not a single calculation, it is a disciplined scientific process. Toxicology data, when used wisely, transforms uncertainty into informed confidence.